Anatomy Of Lungs Biography
(Source google.com)
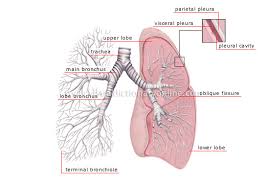
If you are learning patterns of
collapse and consolidation you must learn the lobar anatomy and fissures of the
lung first. One of the difficulties with learning lobar anatomy is that the
descriptive terms (upper, middle and lower) are very approximate to the point
of being misleading. Consider the size and shape of the right lower lobe shown
below. It could have been justifiably named the posterior lobe rather than the
lower lobe! The lobes of the lung are further
divided into segments. If you are a high achiever, you could learn the segments
of the lobes. This can be useful when interpreting consolidation patterns on
plain film chest X-ray images- involvement of different segments of a lobe will
produce different patterns of consolidation.
adapted from By Fred W. Wright
Radiology of the Chest and Related Conditions: Together with an Extensive
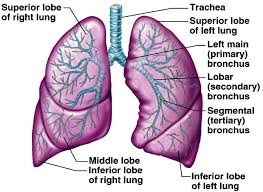
Illustrative Collection of Radiographs CRC Press, 2002 The RUL is comprised of three
segments: apical, posterior, and anterior adapted from By Fred W. Wright
Radiology of the Chest and Related Conditions: Together with an Extensive
Illustrative Collection of Radiographs CRC Press, 2002 dapted from By Fred W. Wright
Radiology of the Chest and Related Conditions: Together with an Extensive
Illustrative Collection of Radiographs CRC Press, 2002The right middle lobe has
two pulmonary segments which are situated side by side; the more lateral
segment, approximates the size of its adjacent neighbor ( medial segment). The
medial segment abuts the right heart border medially , while lateral segment
extends to and comprises a portion of the lateral border of the right lung.
When viewing chest radiographs
with pathology involving the right middle lobe, it is important to think about
the shape and position of the RML in three dimensions. This may not be easy at
first. Note the description of the lobes is very approximate.
adapted from By Fred W. Wright
Radiology of the Chest and Related Conditions: Together with an Extensive
Illustrative Collection of Radiographs CRC Press, 2002The right lower lobe is
comprised of five pulmonary segments. It is a large lobe and will provide
varying patterns of consolidation depending on which segments are involved adapted from By Fred W. Wright
Radiology of the Chest and Related Conditions: Together with an Extensive
Illustrative Collection of Radiographs CRC Press, 2002Note that consolidation
of the apical segment will not result in loss of the diaphragmatic outline.
adapted from By Fred W. Wright
Radiology of the Chest and Related Conditions: Together with an Extensive
Illustrative Collection of Radiographs CRC Press, 2002 n the left there is no
middle lobe; the anatomical equivalent region corresponding to the right middle
lobe is known as the lingula, and like the RML, is also composed of two
segments. Unlike their counterparts on the right however, the segments are stacked
one on top of another, rather than side.
Note that upper lobe pathology could appear very low on a chest X-ray
image. The upper lobe is the anterior lobe as much as it is the upper lobe.
adapted from By Fred W. Wright Radiology of the Chest and Related Conditions:
Together with an Extensive Illustrative Collection of Radiographs CRC Press,
2002By Fred W. Wright Radiology of
the Chest and Related Conditions: Together with an Extensive Illustrative
Collection of Radiographs CRC Press, 2002 There
are probably three commmon relevant factors. The first is that there is
variability in the orientation of the horizontal fissure between individuals.
Of particular relevance is the variability of the hporizontal fissures
horizontalness. Secondly, and possibly more importantly, patients are not
always perfectly erect for PA/AP chest radiography. For example, apart from
normal random variation in the way patients stand, patients with large
protruding stomachs will tend to lean forward for erect PA chest radiography. A
third factor is the presence of disease which either pushes or pulls the
fissure.








Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
Anatomy Of Lungs Lungs Diagram of a Smoker after Smoking Cancer Anatomy And Heart Drawing Images AFter Smoking Wee
No comments:
Post a Comment